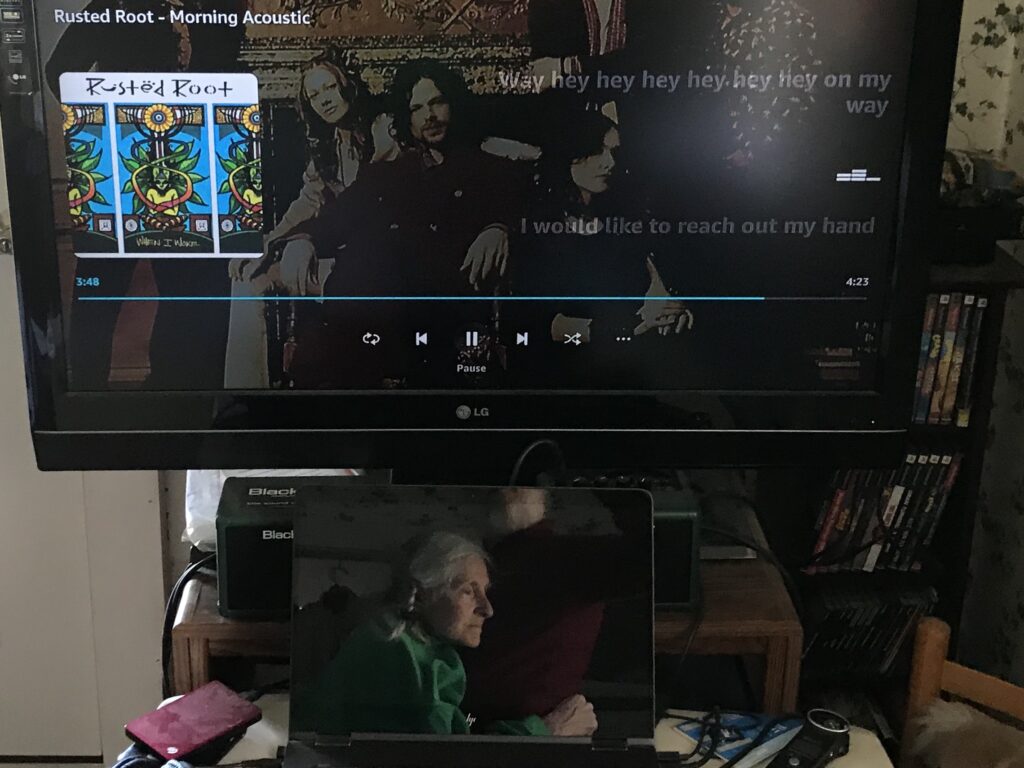
After feeding the cats I return to our “bedroom” to start Cindy’s day. If her eyes are closed, droopy or alert I go about my normal routine. On this day her eyes are fixed on the ceiling in a vacant gaze, giving me cause for concern. Before I get near Cindy I chat about anything that comes to my head. I turn on the music and overhead light for more stimuli in the room. Then as I draw near I announce:
“Hey, beautiful! I’m going to give you a hug. OK? Are you ready for a nice hug? Here I come.”
Whenever I see that gaze in Cindy’s eyes now I go into these precautionary measures. A few weeks ago Cindy also had a vacant gaze in her eyes as I was about to start her day. When I walked right over and hugged her, she immediately went into seizure. Her face turned beet red, revealing intense physical and/or emotional distress.
I continued hugging Cindy while adding soothing words to lessen the seizure. I did not give her lorazepam after the seizure was over since they usually are weeks apart. Plus I have been giving the anti-anxiety medicine only at night; I keep Cindy calm by other means during the day.
A few hours after her wake-up seizure Cindy once again vacantly gazed at the ceiling. I played guitar as a strategy that has worked well in the past. Not this time, though. Her body again went rigid and she started to breath convulsively. I threw the guitar on my bed and rushed to limit the seizure activity from round two.
Now that I am concerned when I see Cindy’s vacant gaze in the morning we have reached another milestone in Cindy’s decline. I gauge her condition by her only tell-tale feature, her eyes. Her vacant gaze indicates some type of internal agitation, occasionally accompanied by spasmodic rigidity of her limbs. This upsets me even when seizure is not the result.
At times Cindy still has alert eyes. She will look around the room trying to make sense of what she sees. Sometimes they follow me or another person around. Sometimes the alert eyes are joined with a smile. Ironically, Cindy becomes most alert for the few days after a seizure, as if she has shaken the fog away from her head.

When Cindy is neither agitated nor alert her eyes are closed or drooping, revealing Cindy to be asleep or barely awake. Another milestone had been reached a few months ago when I let Cindy sleep whenever she wanted during the day. She still sleeps at night as well.
I know what to make of the vacant gaze … that’s bad … and the alert eyes … that’s good. I am never sure what to think or feel about the closed or drooping eyes. Part of me feels relief, even comfort, in knowing that Cindy is at least not going through some internal agitation. I occasionally imagine that she might even be having a pleasant dream. The other part of me recognizes the increased amount of time Cindy has a vacant gaze or sleepy eyes, rather than being alert.
I take pride in Cindy lasting so long in hospice care, now going on twenty months. I take pride in how the nurses and aides still marvel at Cindy’s appetite and skin. I take pride in Cindy’s will to live continuing indefinitely. She cannot become any more nonverbal, immobile or incapacitated than in this final stage of Alzheimer’s, but her appetite, health and will to live remain strong.
Unfortunately, a will to live can prevent dying but provides no remedy for being fully incapacitated, at least not for Alzheimer’s. A will to live does not reverse the declining alertness. A will to live may not even mean life is being enjoyed. Make no mistake, the decline continues. It’s all in the eyes.